
What's the problem with protein in very preterm infants
By Nicholas Embleton in nutrition
· 460 views
I’m still learning about the potential to create an online community of like-minded people interested in improving nutrition and growth in preterm infants, especially in more resource limited settings. But as an introverted academic I struggle to write freely, without constantly over-thinking and feeling the need to continually cite every statement as if writing for academic journals. Anyhow, here goes …

Credit to CNN 2023 for the photo - you’ll need to read the follow up post to understand the meaning of this photo!
In my first post, I discussed the question about whether it’s possible for a sub-1250g baby to grow on breastmilk alone. This is important for resource limited settings where access to PN and nutritional supplements is limited or absent.
The nutritional needs of preterm infants are complex, and they need more nutrients per kg than infants born full term. This is especially true for macronutrients (protein, fat and carbs) and micronutrients such as vitamins, electrolytes, and minerals, and trace elements such as iron, manganese and zinc etc. Given their rapid growth rates, limited stores and excess demands (illness etc.) it isn’t surprising they have high nutrient needs. Defining what is an optimal intake is challenging.
In-utero growth and the placenta
In-utero growth is supported by nutrients transported across the placenta. Lots of glucose and amino acids (to make protein) and essential fatty acids, but relatively lower amounts of total fat compared to life ex-utero. As with all mammals, placental transport is perfectly evolved to ensure optimal growth in an environment that is more hypoxic than postnatal life. Large amounts of amino acids are transported across the placenta, and nitrogenous waste products passed back to the mother for her liver and kidneys to detoxify and excrete. Uterine blood flow is around 500 litres/day in the 2nd trimester and >1000 litres/day in the 3rd trimester, most of which goes through the placental inter-villous space from where nutrients can pass into the fetal circulation.
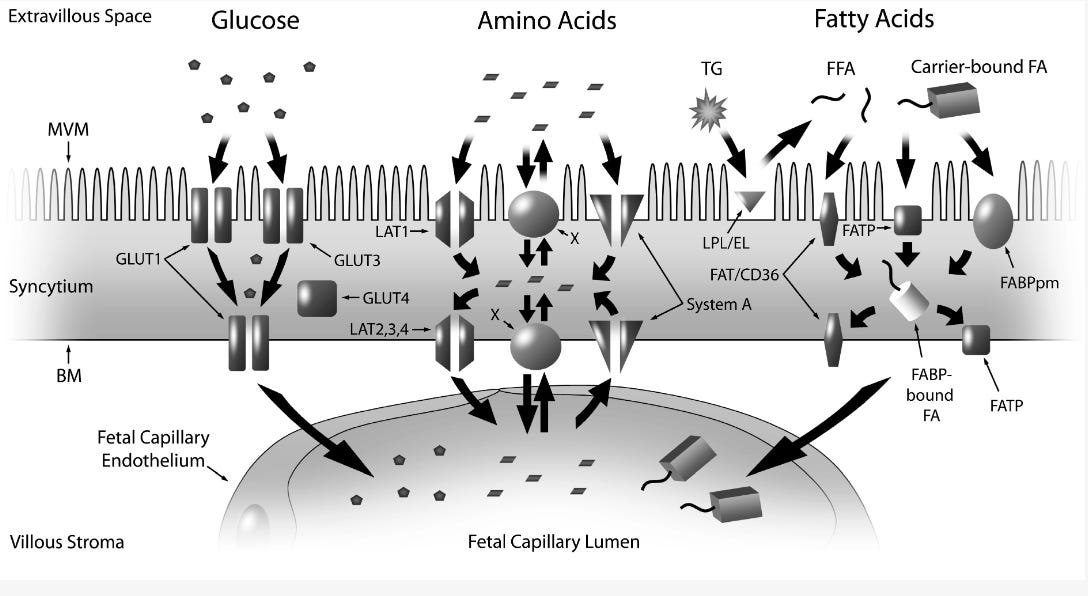
Int. J. Mol. Sci. 2014, 15(9), 16153-16185; https://doi.org/10.3390/ijms150916153
The concentration of essential nutrients like amino acids and minerals in uterine blood therefore doesn’t need to be that high, as the absolute amount that could potentially be provided at those blood flow volumes even with low concentrations is immense. Minerals such as calcium and phosphate precipitate in solutions when the concentration gets too high, but high uterine blood flows solves that problem. When you are restricted to just a total fluid intake of 150ml/kg/day there are challenges everywhere you look to concentrate the solution and provide the optimal balance. We can never provide enough mineral via PN, and we need to get the amino acid composition just right. Enough to grow, but not so high you place a strain on metabolism (autophagy), renal function, and nitrogen excretion. How do we replicate placental nutrient transport when we use PN or start feeds?
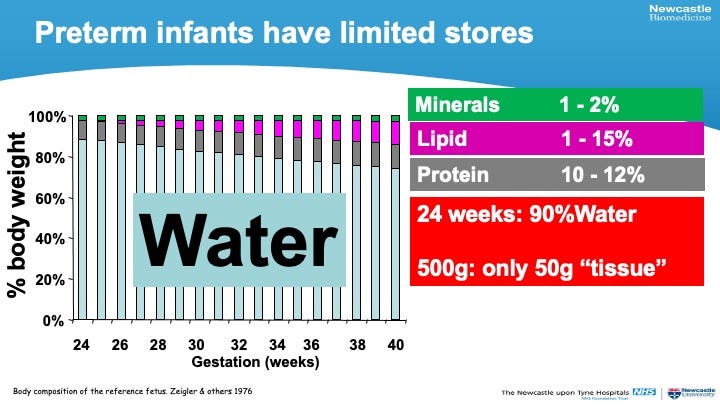
Body composition of the reference fetus
Studies conducted in the 1970s and 1980s used the factorial method which estimated body composition (fat, minerals, protein etc.) at different weeks of [fetal] development, then used subtraction to work out how much of that nutrient was accreted between one week and the next. When you do this for protein you come up with a figure of around 2g/kg/day. However, simply supplying that amount will not lead to growth as there are metabolic inefficiencies and losses. You can’t convert 2g of dietary protein (breastmilk protein or amino acids in PN) into 2g of muscle protein (or liver protein) as it has to be digested, broken down, transported to the liver (as peptides and amino acids), metabolised and then reformed into muscle protein. The amino acid composition of muscle will differ from that of breastmilk protein. There is also continual re-modelling of body proteins even when you are not growing - like you and me. This results in an inevitable loss of ‘protein’ as nitrogenous compounds in the urine (urea) and stool. Several billion gut epithelial cells are lost every day (the whole gut lining is replaced every 6-7 days). All of these losses and inefficiencies add up to around 1.5g protein equivalent, which is why 3.5g/kg/day seems to be the minimum intake for most very preterm infants to grow.
Body composition studies provide a fascinating insight into fetal growth. These early studies show that only 1-2% of body weight is due to mineral in bone, and this is fairly constant over the 3rd trimester. Lipid stores are virtually absent at 24 weeks, although there are lipids in all cell membranes especially neurones, brain tissue and the retina. By 40 weeks, fat content is around 13-14% and double this - 25-30% - by 3 months of age. Protein is fairly constant at 10-12%. If you do the math, you’ll see that most of the weight of a 500g baby is actually just water, so when you care for a 24 week infant, remember there’s only 50g of dry tissue.
Parenteral Nutrition (PN) & the shrinking baby
In parenteral nutrition (PN) solutions there is no protein, just amino acids (essential and non-essential) but we talk about ‘protein’ as it makes it simpler to inter-convert. Because PN does not involve gut (splanchnic) metabolism, losses are lower than enteral, and an intake of 3-3.5g/kg/day is usually enough. With enteral nutrition, studies show that lean mass accretion (lean mass is pretty much everything that isn’t fat) is optimal at around 3.5-4g/kg/day, although some extremely preterm infants may need a little more, perhaps up to 4.5g/kg/day.
https://www.sfnmjournal.com/article/S1744-165X(25)00029-0/fulltext
PN is an essential component of preterm NICU care in high-resource settings, but is unavailable in much of Africa, and other low-income settings. If a baby is not receiving enteral milk in those settings, it is impossible to grow. Furthermore, because of the inevitable recycling of protein, there is still ongoing protein (nitrogen) loss meaning a baby receiving no PN will not simply stay the same weight, but will in fact, shrink. Even when you think you are doing a good job and giving a little PN, if you are only giving 1-2g/kg/day (a good amount to start at) the baby, in all likelihood, is still shrinking.
Why extremely low birthweight babies don’t grow optimally on un-fortified breastmilk
Assuming an ELBW infant needs around 4g/kg/day protein from enteral sources, the question is, how much can they get from breastmilk. Breastmilk protein of course is the highest quality. Quality means the extent to which the amino acid profile meets needs. Highest quality for breastmilk when casein and whey proteins are considered together, a little lower quality for amino acids in PN, and it would be low quality if we used vegetable protein (which of course, we wouldn't). The real challenge though is quantity - the concentration of protein in most Mothers Own Milk (MOM) after the first few days (when lactation reaches ‘full’ volume) is only around 1g/100mL. In donor human milk (DHM) it may be lower (around 0.8g) although there is considerable variability. If MOM is fed at 200ml/kg/day an ELBW may still only get around 50-60% of what they need to grow optimally. It is possible to add extra calories using supplements (MCT, olive oil etc.) and extra minerals, sodium etc. but protein is challenging as it has to come from another animal.
Greek protein only just meets essential needs
Protein comes from the Greek meaning the ‘first order’ - the primary, most important constituent of life. No protein, no life. Given how rapidly infants seem to grow, and the primary importance of protein, why is the amount in breastmilk apparently low? Term-born infants need less protein per kg than preterm, up to 1.5g/kg/day. This means that breastmilk (1g/100mL) meets most healthy term infants perfectly if they drink around 120-150ml/kg/day - but there seems to be no room for error! No spare capacity. And the amount of protein the mother eats makes no difference to the protein content of milk. Nature is very conservative. No wastage. Interestingly, a significant proportion (perhaps 15%) of the nitrogen in breastmilk is from urea. This can be metabolised by gut bacteria (especially certain Bifidobacteria spp), and converted into amino acids providing nutrients for infant growth.
A likely reason that protein is so low comes from understanding infant and child development in complex society. Growth needs to be slow in healthy infants. Unfortunately, this is far from ideal for a ELBW who is desperately trying to grow as quickly as a fetus. A 24 week infant going from 500g at birth to 2500g at NICU discharge 3 months later is a 400% increase. If a term baby born weighing 3.5kg grew this quickly it would weigh the same as a 5 year old (17.5kg) by 3 months age. Low protein is a necessary component of optimal development.
In my next post, I’ll be discussing breast milk protein in different mammals, brain growth and how humans differ from most other mammals. Thanks for the read.
I’d be grateful for your help in sharing this, and the Baby Loss project posts, with others interested in NICU nutrition and/or Baby Loss. I’m not interested in getting likes or views on their own; I’m interested in connecting with others to see if we can improve outcomes, through collaboration, raising awareness, sharing innovations and good practice, and education. Thanks for any shares, re-stacks.
-
 1
1
-
 1
1
Recommended Comments