
-
Sorry to be late to the party. Been busy. NIPPV is mostly a stealth way to increase distending pressure to levels most people are unwilling to use with CPAP. The fundamental flaw with all the studies comparing CPAP and NIPPV is that the mean airway pressure is substantially higher with NIPPV than with CPAP. When compared at the same mean airway pressure, there is no difference in short-term outcomes. Luise Owen long ago showed that very few NIPPV cycles generate a measurable tidal volume. This appears to be because the glottis is not open unless the baby is breathing in. Theoretically, synchronization should help this, but it is not always available or effective. Sherry Courtney's group showed that when used with the RAM cannula there is virtually no generated TV whether in synchrony or not. The RAM cannula is a terrible interface, it is really NOT appropriate for CPAP or NIPPV, it is really just a high-flow cannula (no expiratory limb, must not be occlusive). NIV NAVA is probably the only form of NIPPV that truly works - study is in progress to show that. Some of my colleagues like to use NIPPV. When I take over, I switch to CPAP at the same mean pressure and the baby never notices - except for less gas in the belly..... Cheers, Martin Keszler, Brown University, Providence, RI
-
I can't comment about how well HFOV VG works with other devices, but it works remarkably well with the Draeger VN500 (and presumably the VN800 as well. We completed a 225 subject multicenter safety clinical trial to provide data for an eventual approval by the USA Food and Drug Administration and found that the measured TV was within 0.1ml of set TV in 93% of cycles and 96% when user error was excluded. See attached. And as several posts above indicated, with VG, the TV is fixed, so a change in frequency has no impact on TV (unless reaching the limit of TV in a large baby ventilated at an inappropriately high frequency). So, increasing frequency will DECREASE PaCO2 , the opposite of what you see with HFOV without VG. The easy way to remember is that it now behaves like conventional ventilation: faster rate = more CO2 is removed. 2019 DOVE VG Does it work Poster_ Final.pdf
-
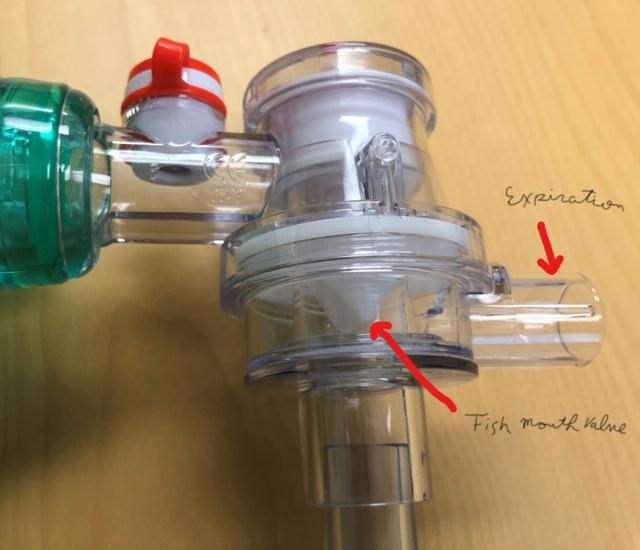
Be careful when using large filters, as this adds very large dead space to the system whey using the T-piece resuscitator (e.g. NeoPuff - see first pic). Exhalation occurs via the opening of the PEEP valve at the top, so the filter is in-line. With mask ventilation, there is probably enough leak around the mask to wash out the dead space, but if used in an intubated baby, you would likely have significant dead space gas rebreathing with hypercapnia. With most self-inflating bags the filter can be placed on the expiratory limb as shown in the second picture, therefore there is no added dead space. Detail shows the fishmouth valve that directs expired gas to the filter and PEEP valve. So, until you can get your hands on neonatal filters, you might be better off using a SIB, despite the other problems. Smaller filters are available and should be OK to use with the T-piece.


-
I have observed this repeatedly in babies whose mothers were taking SSRI antidepressants, specifically Zoloft. Happy baby who does not cry. Cheers, MK
-
Great question, Juan Carlos. I am partial to the VN500, but I'm sure both devices can deliver VG quite well. The problem is that babies don't like to be acidotic. Consequently, there is a problem with permissive hypercapnea in the first days of life in small preemies, because their kidneys are not able to compensate for respiratory acidosis. Therefore, the baby will try to generate a tidal volume sufficient to bring the PCO2 down and normalize the pH. As you know when the tidal volume exceeds the target value, PIP will come down and pretty soon, your baby may be on endotracheal CPAP with rising oxygen requirement (due to the drop in MAP), tachypnea and increased work of breathing. You would have to sedate the baby sufficiently to suppress their respiratory drive, which is a bad idea. People find all kinds of ways to reduce the support for the baby's effort, for example changing from AC to SIMV at a low rate, so the baby is unable to generate adequate minute ventilation and correct the acidosis. So, the baby is struggling, but the doctor is happy, because the PCO2 is where he or she wants it. If you can buffer the acidosis by adding some acetate to your TPN and get the pH up to near normal, you might be able to let the CO2 rise gradually. The focus needs to be on pH, not PCO2, because it's the pH that is the primary stimulus for respiratory drive. Basically it is better to support the baby's effort to maintain normal pH and avoid the mistake of looking only at the PCO2. Ultimately, it is the perivascular pH that controls cerebral circulation, but unfortunately all studies keep focusing on PCO2 and ignoring pH. What we know is that rapid fluctuations in PCO2 confer the greatest risk of IVH. Once the baby is a bit older and the kidneys are more mature, it'a s lot easier to allow permissive hypercapnia if they still need mechanical ventilation. I hope this helps, MK
-
Effect of instrumental dead space.pdfEffect of instrumental dead space.pdfYour first option is the correct one (I assume that though you asked about a 400g baby you used 0.5 kg in your calculations, so we really are dealing with a 500g baby). In any case, the effect of the added dead space is already figured into the approx. 6ml/kg. The concept of dead space is a bit relative. It has an effect, but not as large as you would think if conventional physiology strictly applied. There clearly is some admixture of fresh gas and dead space gas so adding the entire dead space to the calculation would result in overventilation. Please see the following publications that address this issue: Nassabeh - Montazami S, Abubakar K, Keszler M. The Impact of Instrumental Dead-space in Volume Targeted Ventilation of the Extremely Low Birth Weight Infant. Pediatr Pulmonol. 2009;44:128-33. Keszler M, Brugada M, Abubakar K. Effective Ventilation at Conventional Rates With Tidal Volume Below Instrumental Dead Space: A Bench Study. Arch Dis Child Fetal-Neonatal Edition 2012;97:F188–F192 Hurley EH, Keszler M. Effect of inspiratory flow rate on the efficiency of carbon dioxide removal at tidal volumes below instrumental dead space. Arch Dis Child Fetal Neonatal Ed. 2017;102:F126-F130. doi: 10.1136/archdischild-2015-309636. PubMed PMID: 27515984. Cheers, Martin Effect of instrumental dead space.pdf Effect of flow rate on CO2 elimin ADC FN 2016-Hurley.pdf
-
@spartacus007: Sorry for slow response. Yes we would use AC and avoid heavy sedation. Only use paralysis if despite good NG tube placement we are unable to keep gut decompressed, meaning we use it rarely. Evidence-free zone, for the most part, but muscle relaxation has many downsides and I am a believer in making the baby breathe as much as they can, which minimizes intrathoracic pressure and adverse hemodynamic consequences of PPV. As for SPO2 target, the goal is NOT 100%. Gentle support with minimal PIP needed to get the heart rate up and SPO2 into the low 90s. Generally start with FiO2 around 0.6 and wean if SPO2 is >92-93%. @bimalc : We do not use cuffed tubes, though it would be appropriate if you did not have a ventilator that has excellent leak compensation capability, like the Draeger VN 500, which can accurately compensate for leak of up to 60-70%. If you have a leak anywhere near that large, the baby need a larger tube. @tarek: I love the HFOV + VG. It works very nicely, but in the USA, the HFOV option is not yet approved by the FDA, so I was only able to use it in the context of our preeemie study that will hopefully lead to approval. Given that CO2 removal with HFOV is proportional to F x VT squared, the ability to maintain a constant VT in the face of changing lung compliance is particularly attractive. In my 27 babies we used it on it worked beautifully! Cheers, Martin
-
"We also start on AC-VG. We bring the ventilator into the delivery room and once intubated, get them on to volume ventilation and avoid as much t-piece or bag ventilation as possible. Initial settings are PEEP 5-6, 4-5mL/kg tidal volume, back up rate of 40, and iTime 0.3" Nathan's approach above is a lot more evidence-based than the earlier post from Winnipeg. There is good evidence that relatively low PEEP should be used to avoid over-expansion of the hypoplastic lungs, which contributes to PPHN (Guevorkian, et al, J Pediatrics 2018). The results of the VICI trial also strongly indicate that high distending pressure is detrimental. For some reason (maybe someone will comment on the rationale, I can't think of one) the investigators chose to use an aggressive lung recruitment strategy with HFOV and a gentle, low PEEP strategy with conventional ventilation. The outcomes favored conventional ventilation over HFOV, but that is because the WRONG strategy was used with HFOV, IMHO, not because HFOV is inherently bad for CDH. We looked at the VT needed to keep a normal PCO2 in CHD and found it to be 4.5 ml/kg. These were data from fairly long ago, when we targeted normal PCO2 in low 40s (Sharma, et al, Am J Perinatol. 2015). 4ml/kg is probably appropriate when aiming for mild permissive hypercapnia. Babies with CDH have the same rate of metabolic CO2 production as any other baby that size, so they need roughly the same alveolar minute ventilation, even if their lungs are small. 3ml/kg would be unlikely to work, since that is the volume of anatomical and instrumental dead space. But I know people who use 3ml/kg because you have a large ETT leak and are not using leak compensation, so that the real VT is around 4ml/kg, but they don’t realize it. Thanks, Martin Keszler MD Professor of Pediatrics, Brown University
-
-
John, I have collected some data on this subject with colleagues from Japan and Poland, who have been using HFOV with VG on the VN 500. We have two abstracts at the PAS meeting in Vancouver on this very subject, so please come to Vancouver and find out. Or read the abstracts when they come out. The data are focusing on what VT is needed for normocapnia, not specifically on safety, because using VG should increase safety of HFOV by avoiding inadvertent hyperventilation. Stay tuned, Martin Martin Keszler, Brown University, Providence, RI
View in the app
A better way to browse. Learn more.


