.jpg.0241c805f885be5fcfba0a960300da57.jpg)
Everything posted by Vicky Payne
-
 https://hubble-live-assets.s3.amazonaws.com/bapm/attachment/file/353/DA_framework_final_October_2020.docx.pdf
https://hubble-live-assets.s3.amazonaws.com/bapm/attachment/file/353/DA_framework_final_October_2020.docx.pdf -
-
 Developed by the Burdett Trust, a mind toolkit has been developed by nurses for nurses, however, many of these resources would be useful for any clinicians looking to improve their own personal well-being and develop leadership skills. Sections include resources on managing conflict, inclusivity and diversity and relationships.
Developed by the Burdett Trust, a mind toolkit has been developed by nurses for nurses, however, many of these resources would be useful for any clinicians looking to improve their own personal well-being and develop leadership skills. Sections include resources on managing conflict, inclusivity and diversity and relationships. -
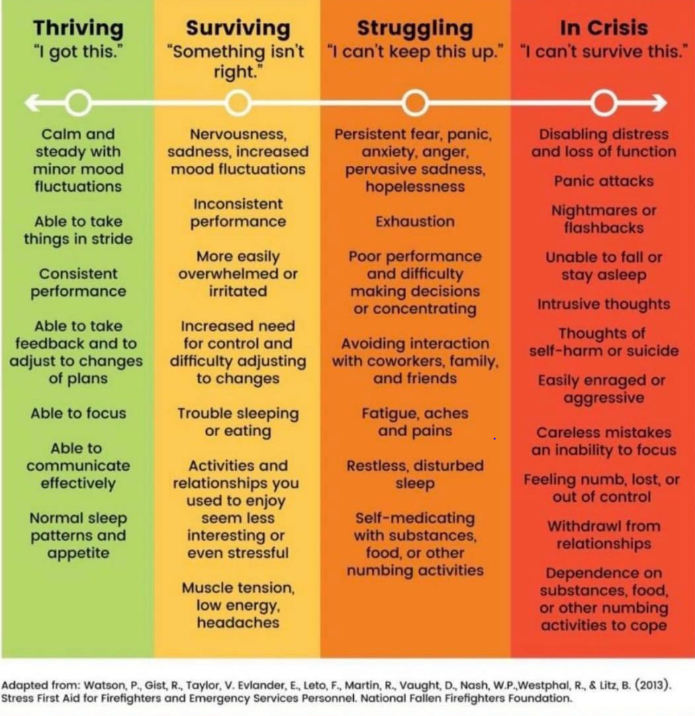
Thank you for your openness and honesty. I think you will not be alone at all in feeling like this, particularly at the moment. I do not know what it is like in the US, and I can only share my perspective as an ANNP, but the first step is to be able to reflect and recognise and it sounds like you have had the insight to do just that. In fact, in a way, it is good you have colleagues around you who feel able to raise such difficult conversations with you. Personally, the complex systems we work in do make this hard, and I agree that pressures have become "normalised"- this is a great article for considering how healthcare professionals adapt constantly to prevent errors, but the constant staying late, skipping meals, working overtime e.t.c that we do to adapt for the system can take its toll: https://qualitysafety.bmj.com/content/28/8/667 There is an increasing amount of literature about physician and nursing burnout. I also think 'we' that make policies and guidelines and monitor safety etc need to think more about how we help our staff to do the job they want to do, rather than just "fire-fighting". I also really like this infographic- some on Twitter have suggested putting this in staff rooms for people to put stickers (anonymously) next to how they are feeling. I have fluctuated between "surviving" and "struggling". I found opening up and being honest to those that could help, instantly made me feel better even though nothing had changed. Instead of staying off social media, I found re-engaging with others helped. You are not alone. And you have insight, which is the first step in recovering 🙂 I hope you get to take some time to rest @Stefan JohanssonI am also better at working than relaxing! I think the culture of "being busy" or equating success with being busy, is also problematic. I also come from a "strong work ethic" background 😉
-
-
What do you mean by placing them incorrectly? What is interesting is that the original formulas developed in 1960's were developed to have the catheter in the right atrium, what we now know to be unsafe- recent review on methods to calculate insertion length here: https://www.tandfonline.com/doi/full/10.1080/14767058.2020.1838478?casa_token=yLqwwr0MfEUAAAAA%3AJxsgcDBkqa3owb5sDwdIOtr-tITC-MA56taD1smV0xqhNdjOjjJX50HekBWaE-ck1FgZrDb5tZPz I agree with @Francesco Cardona that POCUS is the way forward here, though we are not currently using it routinely either....
-
-
Signed up too!! I think this is going to be a great step for the 99NICU forum 😊
-
Thanks- we do some of these things (in principle!) 1. Change TPN using "surgical ANTT" but not with a hat or mask. We have lots of "traffic" in our nurseries, though recently we have moved to preparing the fluids in a separate room to avoid this traffic (doesn't appear to have made much difference to our rates so far) 2. Yes, we have these 3. We try to do this, though I am not sure how well it is adhered to. We do try to avoid putting any medications via central lines i.e caffiene, fluconazole but I think that infusions such as morphine/KcL piggybacks, inotropes e.t.c may get changed at different points in the day sometimes when it is busy, rather than waiting till the TPN is changed. 4. We don't do this! What do you think is the benefit of this over inserting a central line? How many beds do you have (just by way of comparison)? Do you do surgery? We do not have very many months of zero. Zero is the rarity or the outlier for us!! We have a mixture of pathogens such as Staph aureus and gram negatives, but also plenty of CoNs- staph capitis, epidermis e.t.c Thanks for the suggestions 🙂 Best wishes, Vicky
-
Hi! Thanks for the tag Stefan. I think on the whole we would put up brand new TPN onto a new long line, though on some rare occasions other fluids may be switched from UVC to Long line. Central to central generally accepted as ok, peripheral to central a clear no, no! However, we are lucky to have standardised stock TPN bags kept on the neonatal unit, so we have easy access to this, and once warmed we can attach immediately with no waiting around - we only have to wait till the evening for bespoke TPN. We have salt free vamin for first few days, and then we have a preterm and term bag. We would try to avoid long periods of additional 1ml/hr of saline running in the smaller/ELBW babies, due to the additional fluid volume and salt. We have switched back to Scrubbing the Hub technique over alcohol impregnated caps which (spoiler alert) made no difference and cost us almost £10, 000 a year- abstract submitted on this just this week so watch this space! However, our rates are not low (though we don't use the CDC definition which I think is more specific about "infection from another location") and despite multiple efforts, our central line sepsis rates have not really changed much over 5 years, so I cannot claim to know the right thing to do! However, if you would be willing @MVNICU I would love to organise a conversation with you about your setting, your local practices and your zero rates. It would be really helpful for us 🙂
-
The NOTE programme (collaboration between ESPR and University of Southampton) are opening a Pharmacology module in June, led by Karl Allegaert and Sinno Simons, using virtual/remote teaching. More information in attachment and via link below 🙂 https://www.espr.eu/news/news-detail/e-learning-neonatology-paediatrics/186 Proposal NOTE module DINA4 v3 (1).pdf
-
There has been a recent narrative review of cooling outside of "standard" criteria here: https://www.sciencedirect.com/science/article/abs/pii/S1355184118301595 I agree with above comments- I think given need for resuscitation at 10 mins (ventilated) and evidence of encephalopathy on clinical assessment (+/1 aEEG/CFAM) then we would have cooled on admission. We generally do not cool > 6 hrs but have on occasions, including late preterms. We had an interesting situation a few years ago where a baby ended up being resuscitated after an unplanned extubation (ex-preterm, difficult to get chest movement, difficult to intubate, long period of bradycardia and poor oxygenation) and there was a decision made to cool. What happened in your case?
-
I really liked this blog post! I guess many of us have seen devastating cases of post-transfusion NEC that stay with us and therefore add "bias" to our judgements on this topic. There are still questions though right? Like the severity of the anaemia (how low do we leave the Hb and is that threshold different for certain babies?), the duration of anaemia (how long do we leave it before we transfuse?) and then, if the mechanism is a re-perfusion injury post-transfusion, how do we prevent it?!
-
Thanks for the share- this had been on my to-listen list. The article is an interesting read as well (link below). I am interested in the Staffing Models of high performing NICUs which include: "Neonatologists rounded on fewer patients, less nurse turnover, better nurse: patient ratios and neonatal nurse practitioners rounding on VLBW infants" Definitely someone for next years line up 😉 https://fn.bmj.com/content/104/1/F13?rss=1&utm_source=feedburner&utm_medium=feed&utm_campaign=Feed%3A bmj%2FqEtm %28Archives of Disease in Childhood - Fetal and Neonatal Edition current issue%29
-
Of course! I have attached a publication of the work done at Southampton, which includes the nutritional assessment tool- I do not think there is anything there that would be too surprising, but it does mean that our late preterm/term infants do not get stuck on the same feed increases as ELBW, or really slow establishment of feeds. The nurses use this tool on Monday night shifts, ready for our nutrition ward round on Tuesday mornings. This specialist ward round comprises of Consultants, Neonatal pharmacist, Dietitian and surgical representatives. Hope it is helpful. 🙂 My question back to the group: How do people feed babies (or not!) with HIE undergoing Therapeutic Hypothermia.......??? Johnson_et_al-2015-nutritional screening tool.pdf

-
Hi Karsten, In Southampton, UK, we have a nutritional screening tool (high risk, medium risk, low risk) which guides us for increasing feeds. ELBW infants would be increasing between 10-20mls/kg/day of EBM. We usually start colostrum as available, then 0.5ml/ 4 hourly, increasing in 10-20mls/kg/day volumes. We are trying to start breast milk fortification at 100mls/kg/day though mostly at 120mls/kg/day. I hope this is helpful. Speed of Increasing Feed trial results later this year may also help guide practice. 🙂
.thumb.jpg.9337b79d733812b332433aa8f037f9b8.jpg)

