
-
Hi @Bonnie , we rely on visual assessment by physiotherapist. They have made a parents’ folder called “Back for sleep, tummy for play.” I don’t have the PDF version, but would you like me to ask for it as a PDF? It’s in Swedish though 😀 And of course, when there is a back head asymmetry, the PTs give specified advice how to use back support, stretch torticollis (if any) etc. They also plan and do follow up themselves. Would be great to hear more about the more advanced technologies, are they in use in nearby units? And esp why/how they are used?
-
I would argue Yes. We analyse mothers own milk and all donated bank milk and fortify up to approx 4g protein/kg/d
-
AI is the new cool kid in town. While I get the principal impact of AI, and have some very limited experience (with free versions, and mostly as a Google replacement), I guess AI could have some applications in our daily practise as clinicians and researchers. So, I want to learn from you whether you use AI professionally as a clinician/researcher, and if so, what do you do, practically speaking? What tools do you use for what? Please share ⤵️ !
-
@Annika thanks for sharing about this! I am on vacation this week but will see if I can connect 😀
-
Thanks for sharing, just read your case report, great presentation of this rare complication. My experience is really limited, and is restricted to the first two columns (non-pharmacological and heparin-like anticoag)
-
Yes, as clinicians, we need to diversify the principles and the practices. And thats where I disagree with Prof Lagercrantz - while his reasoning is interesting, it offers little (or no!) guidance in the actual care of really tiny patients. And yes, we are indeed caring for minds in the making, what is the best things to do, we may never know, but we shall feel an obligation to keep looking for that.
-
Thanks @Mariana Oliveira for sharing this. Hugo Lagercrantz, neonatology professor emeritus at Karolinska, reasons a lot about when the consciousness is formed, like ~when you become a conscious person. He uses this chain of arguments also for how/when to practically define the window of viability, i.e. that infants at 22 weeks are not yet full-fledged individual (although the legal definition of "live born child" is 22+0 weeks in Sweden) While I disagree a bit on his reasoning, I think there are some points, and especially how to keep the normal trajectory for the developing brain.
-
Thanks for sharing a great post, it makes me think about how many of us think about families, and having children. Also when a singleton infant (or older child) dies, I often hear someone in staff asking/saying something about "was it the first-born?" "do they have other kids" etc I just recently heard it after a dramatic event in a NICU. IMHO I think the death of a child is an equally hard experience itself and as such, however the family looks like. And that there is no "economy of scale" in this.
-
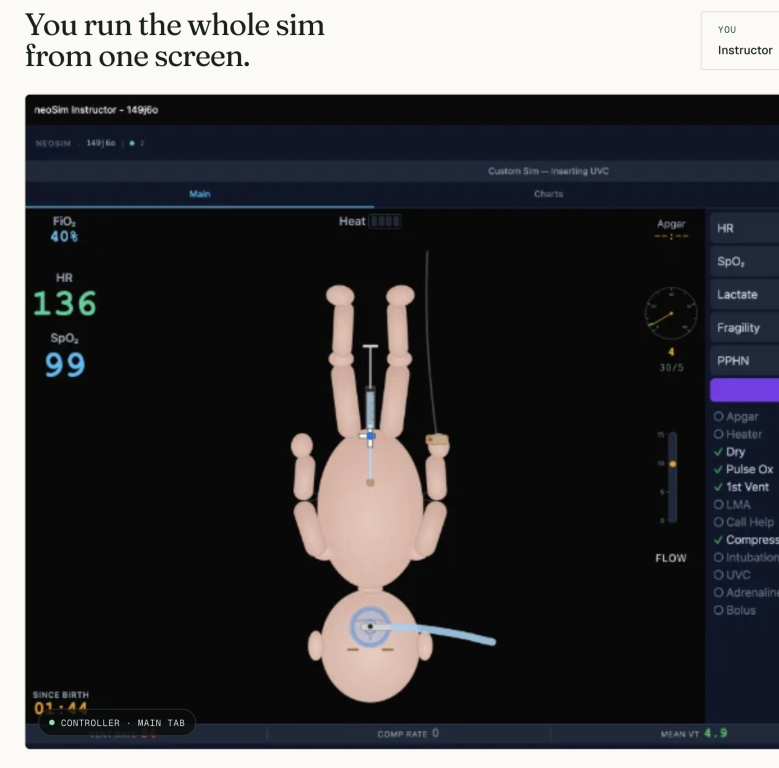 Neonatal resus sim sessions can teach preparation, teamwork, and communication while participants practise the standard algorithm skills and sequencing. We present a new format for this teaching: in person but online, highly interactive, instructor-led but supported by a real-time physiology engine that manages the evolving vital signs on the instructor's behalf.
Neonatal resus sim sessions can teach preparation, teamwork, and communication while participants practise the standard algorithm skills and sequencing. We present a new format for this teaching: in person but online, highly interactive, instructor-led but supported by a real-time physiology engine that manages the evolving vital signs on the instructor's behalf. -
Seems like a fantastic project! Will share in our clinical teams and try out.
-
Hi @Nicholas Embleton it is simply great that we can help sharing your writing here, you have so much experience and knowhow that deserves a wide audience. I hope we can help with a large outreach through our community. Looking fw to a lot of food for thoughts!
-
We also have these around, but very rarely used. We also simulate yearly, but rarely the use of IO-device, room for improvement there. IMHO though, in just newborn infants, there are enough option for intra-vessel catheters. But of course also good with a last resort technology. Given one knows how to use it 🙂 On special occasion was an infant in our late GBS sepsis outbreak some years back (published here: https://pubmed.ncbi.nlm.nih.gov/30152878/). Those very sick infants were all beyond the option for umbilical catheters, and once a colleague used our IO-device, I think a life-saving choice for that particular infant.
-
Hello! I have little to add to Dotans excellent post above, just how we do this - we rarely use immunoglobulines but sometimes opt for this, when there is a DAT-driven hemolytic hyperbili. We typically give 1g/kg, and start the infusion at 0.3 ml/kg/hour, doubling the infusion rate every half hour up to a max of 4.8 ml/kg/h. So, we end up with a total infusion time of about 3.5 hours. I attach the XLS-sheet we use , I am sure you can translate with an AI-engine or so Privigeninfusionsschema-4.xlsx
-
Sweden is a good country to be born extremely preterm. Neonatal intensive care is centralized and pretty much equally organized, and outcomes are regarded as good and similar throughout the country. Like in most other European countries, the welfare system enables equal access for all, practically at no cost for families. Sweden has been at the forefront of the slide of the ”window of viability”, i.e. at which gestational age extremely preterm infants are offered intensive care. I don’t know how this came about, but I think we, i.e. Swedes, have an unusually high trust in society and experts, and we seem willing to ”try and see how it goes” as we count on societal support if problems arise later. If you want to see this from the another angle, one could also regard the Sweden as a bit patriarchal, where people follow top-down advice and form their own opinions and decisions to a lesser extent. As of today, our cutoff between miscarriage and live-birth is at 22+0 weeks, and our national guideline from our Neonatal Society states that mothers with threatening delivery at 22 weeks should be transferred to a regional university hospital and active care should be considered. This current strategy is however on the radar for re-evaluation. The Swedish National Council on Medical Ethics, an independent body within the Government offices, recently issued a thorough report about the care of infants born at 22 weeks. The main take homes are that 1) comfort care without a life-saving intent should be the primary strategy, and that 2) parents have a right to be engaged in a true shared decision-making process. The Council suggests that the Swedish National Board of Health should develop a new national guideline taking their conclusions into account. While this medico-ethical report have already been discussed a lot, even in national public media, I foresee this is only the preamble to a more challenging and painful (and potentially dirty!) debate between the opposing sides of this fence. There will be different opinions and arguments not only from professional representatives and parents, but also politicians, philosophers and many other stakeholders will probably express their various positions. Whether that future debate will be in the best interest of infants born at 22 weeks, we’ll see. With this long introduction, I would like to high-light this paper in Journal of Pediatrics, about Quality of Life in Swedish adults born extremely preterm. In short, the paper is based on the so-called ”1000g-study” including a cohort of ELBW infants born in Sweden in 1990-92. While the paper reports more disabilities in adulthood in those born ELBW, the perception of quality of life was no different compared to a term-born control population. And the press release concludes that ”..these findings provide the best available assessment when giving information today to parents of extremely premature children...” If one only reads the press release and abstract, it all sounds good! But can those findings really be generalized to extremely preterm infants born today? I doubt that. First of all, as shown in the study population flow chart, only half of the eligible survivors completed the QoL survey (168 of 345). If one goes to the Tables, the responders seems to be a much healthier subpopulation, at least there are big differences in disability rates between responders and non-responders. For example, - cerebral palsy was twice as common in non-responders (14.1% vs 6.5%) - epilepsy and visual impairment was four times more common (9.4% vs 2.5%, and 4.7% vs 1.0%) - non-responders had two-three times more often intellectual development disorders (17.1% vs 4.5%), attention disorders (18.8% vs 9.5%) and autism (15.9% vs 6.0%) So, even if the QoL surveying of responders had good internal validity, there are good reasons to question the external validity. Would non-responding ELBW adults with much higher rates of neurological diagnoses score their QoL as high as healthier group responders? The truth is that we don’t know. The main question when it comes to generalizing to today’s ELBW context is however something else, related to a more basic fact. Who are the survivors in the Swedish ”1000g-study”? Neonatal intensive care has indeed improved since then. Today, there is generally a high chance to survive extremely preterm birth. In infants born at 24 weeks and onwards, survival is what we expect, right? But what was the survival in ELBW infants in the early 1990s? The original publication of the ”1000g-study” illustrates how much different the situation was in the early 1990s, see the mortality rates per gestational week in the graph. The overall infant mortality rate was 48% in infants born at 23-27 weeks, and the subgroup of 23-24 week infants had a 80% mortality rate. Furtermore, quite many infants were coded as still-born these days, and one can wonder about the degree of potential mis-classifications there. For example, in week 23, there were 47 live-born (of which 43 died during infancy) and 76 infants were classified as still-born. Naturally, the original cohort included no infants born at 22 weeks. So, the way I read the paper about QoL in ELBW adults born in the early 1990s, is mostly that the outlook is fine for those born at 26-27 weeks, especially in those not impacted by significant neurological morbidities later in life. Which is indeed re-assuring, those infants represent the largest group of extremely preterm infants. However, there remains such a large gap of knowledge about the long-term trajectories for our ”nano-preterm” infants in our NICUs. The sloppy saying goes that ”More research is needed”, but in this case we have an obligation to aggregate structured long term data about health and disease in those surviving the ”window of viability”. Without knowledge, we will keep struggling how our actual clinical work can align with the best interest of our most vulnerable patients and their families.
-
View in the app
A better way to browse. Learn more.



